Strahlenschäden beim Menschen
Eine Bewertung von Joachim Gruber
Die Frage nach der Schwere der Strahlenschäden durch Fukushima
und insbesondere nach dem Wahrheitsgehalt unserer Informationsquellen
Vorwort:
Das Thema wird in zwei Lagern diskutiert. Die Wissenschaft scheint bei weitem noch nicht abgeschlossen zu sein.
(*) Lager 1: Strahlenschäden beschränken sich auf Krebs und Erbgutschäden.
Hier finden sich die Institutionen des nuklearen Establishments, also die International Atomic Energy Agency (IAEA), die International Commission on Radiological Protection (ICRP) und World Health Organization (WHO). Deren Einschätzungen berichtet die Presse, und auf ihr basieren auch die medizinischen Facharbeiten des nuklearen Establishments. Die Strahlenschutzgrenzwerte sind von der ICRP explizit so angesetzt worden, daß Nuklearmedizin und Nuklearindustrie möglich sind.
(*) Lager 2: Strahlenschäden erfassen den gesamten Körper.
Hier finden sich die Nuklearkritiker.
Bisher ist ein Problem, daß die Beiträge des Lagers 2 eine schwache naturwissenschaftliche Basis haben, ähnlich wie die alternative Medizin. Die wissenschaftliche Diskussion ist nicht abgeschlossen.
Wikipedia lief zur Zeit seiner Anfänge nach meinem Dafürhalten auch Gefahr, in eine solche Nische zu geraten. Daß Wikipedia so verläßlich geworden ist, liegt nach unserer Meinung daran, daß sich so viele Menschen unentgeltlich beteiligt haben. Darauf geht Micah Sifry ein: The Impact of Social Web Technologies, breitband, Deutschlandradio Kultur, 12.2.2011 (im Cache, Transskript).
Ich würde die Äußerungen des Lagers 2 als warnenden Gegenpol zu denen aus Lager 1 werten. Im Anhang gebe ich drei Lager-2-Antworten (I - III) auf die Frage nach den Schäden durch den Unfall in Tschernobyl.
Der Schaden in Fukushima wurde bisher nur in Lager 1 quantifiziert. Diese Bemessung wird in Lager 2 als Spitze des Eisbergs bezeichnet.
I. Chernobyl: Consequences of the Catastrophe for People and the Environment
Janette Sherman hat einen Report aus dem Russischen übersetzt, in dem 3 russische Herausgeber mehr als 5000 russische Berichte zusammengefaßt haben. Die New York Academy of Sciences hat ihn (vor Fukushima) publiziert:
Chernobyl: Consequences of the Catastrophe for People and the Environment, Wiley Blackwell (2010).
Alexey V. Yablokov (Editor), Vassily B. Nesterenko (Editor), Alexey V. Nesterenko (Editor), Janette D. Sherman-Nevinger (Editor)
look inside the book
Darin stellen die russischen Autoren fest, daß bisher mehr als 1 Million Menschen an den Strahlenschäden nach dem Unfall in Chernobyl gestorben sind.
|
|
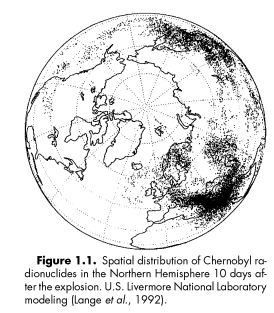
Quelle: Figure 1 in Lange, R., Dickerson, M.H. & Gudiksen, P.H., Dose Estimates from the the Chernobyl Accident, Nucl. Techn. 82: 311-322, 1987. UCRL-96934 Preprint, CONF - 871101 -- 78, invited Paper, American Nuclear Society 1987 Winter Meeting, Nov. 15-19 in Los Angeles, CA.(in cache), reprinted in Alexey V. Yablokov,Vassily B. Nesterenko, Alexey V. Nesterenko, Chernobyl: Consequences of the Catastrophe for People and the Environment
|
Helen Caldicott hat in einem Interview mit Janette Sherman formuliert: "Wir sehen erst die Spitze des Eisbergs." Und das habe hauptsächlich folgende Gründe (wie ich aus dem langen Interview herausgehört habe):
-
die lange Latenzzeit der Gesundheitsschäden durch niedrige Strahlendosen,
- die Vielfalt der Gesundheitsschäden,
- die Absprache zwischen der WHO und der IAEA darüber, was man als Strahlenschaden anerkennt.
II. Vorläufer-Bericht zu 1
The Chernobyl Catastrophe: Consequences on Human Health (im Cache)
Herausgeber: A. Yablokov, I. Labunska, I. Blokov,
Report editiert von D. Santillo, P. Johnstone, R. Stringer, T. Sadownichik
Greenpeace 2006
III. Tschernobyl-Konferenz in Berlin, 2011
Meine Zusammenfassung sind Auszüge aus
"25 Jahre Folgen der Tschernobyl-Katastrophe: Bilanz gesundheitlicher und ökologischer Schäden"
Internationaler Kongreß, 6. - 8. April 2011, Berlin (im Cache)
Herausgeber: Gesellschaft für Strahlenschutz e.V.
IV. UN Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) Reports
UNSCEAR 2008 Report:
"Sources and effects of ionizing radiation"
Volume I
(in cache, cached corrigendum) comprises the main text of the 2008 report to the General Assembly ( A/63/46) and 2 scientific annexes:
- Annex A - Medical radiation exposures; and
- Annex B - Exposures of the public and workers from various sources of radiation.
Volume II (in cache)
comprises the remaining 3 scientific annexes:
- Annex C - Radiation exposures in accidents;
- Annex D - Health effects due to radiation from the Chernobyl accident; and
- Annex E - Effects of ionizing radiation on non-human biota.
UNSCEAR 2006 Report:
"Effects of ionizing radiation"
Volume I
(in cache, cached corrigendum) comprises the main text of the 2006 report to the General Assembly ( A/61/46 + Corr.1) and 2 scientific annexes:
- Annex A - Epidemiological studies of radiation and cancer; and
- Annex B - Epidemiological evaluation of cardiovascular disease and other non-cancer diseases following radiation exposure.
Volume II
(cached corrigendum) comprises the remaining 3 scientific annexes:
- Annex C - Non-targeted and delayed effects of exposure to ionizing radiation;
- Annex D - Effects of ionizing radiation on the immune system (for details see below); and
- Annex E - Sources-to-effects assessment for radon in homes and workplaces.
UNSCEAR 2006 Report - Volume II,
ANNEX D: Effects of ionizing radiation on the immune system (in cache)
The scope of this annex includes reviews of:
- Radiation-induced alterations of the immune response, including immunosuppression (depression) or immunostimulation (activation);
- Possible mechanisms by which the immune system is altered following exposure to ionizing radiation;
- Epidemiological assessments of immune system alterations in various diseases, with emphasis on the
effects of ionizing radiation.
L. Summary (pages 144-150)
346. There are many mechanisms potentially involved in radiation-induced alterations of the immune system:
- Radiation-induced apoptosis is a key mechanism, well established for blood-circulating white cells,
mostly lymphocytes.
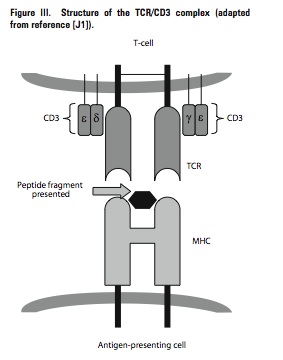
- Mutations of T-Cell Receptor (TCR) genes is a radiation-dose-dependent mechanism which can produce defective TCRs and alter the discrimination between "self" and "non-self".
- There is still some controversy regarding the functional cytokine secretion pattern of helper T-cells following exposure to ionizing radiation, although it is likely that the homeostatic balance between Th1 pattern (cell-mediated immunity) and Th2 pattern (humoral immunity) is shifted towards a pro-inflammatory profile.
- Delayed effects, e.g. bystander effects and genomic instability, have been demonstrated after exposure of the immune system to ionizing radiation. However, the potential impact of such delayed effects in humans is not known.
- Inflammation resulting from the effects of ionizing radiation can be observed at the microscopic level and involves immune cells within and around tumours, but inflammation may be large enough to produce significant alterations of parameters in blood samples. Inflammation may be associated with chronic diseases.
- There is a vast literature showing that immune cells after exposure to ionizing radiation show abnormalities that are quite similar to those observed in normal ageing. These observations at the biological level have so far not been linked to diseases.
- Alterations of the process of antigen presentation at the level of the immunoproteasome have been demonstrated and are possibly a signal of immunosenescence after exposure to ionizing radiation.
- Ionizing radiation can contribute to a disturbance of self tolerance and consequently can pave the way towards autoimmunity.
- Finally, the immunological response against foreign antigens implies T-cell homeostasis, which is disturbed after exposure to ionizing radiation.
click on figure to enlarge
Figure: Structure of the TCR/CD3 complex.
Source: UNSCEAR 2006 Report - Volume II, ANNEX D: Effects of ionizing radiation on the immune system
|
Perturbation of immunological homeostasis
308. Immunological homeostasis is the mechanism by which the immune system responds to foreign antigens (e.g.
an infectious organism) and then returns to its original state, although retaining memory cells that will protect the host
against subsequent infection by the same organism. This homeostasis is achieved in the T-cell system by the balance
between renewal and death of naive and memory T-cells. The ability to maintain both naive and memory T-cell pools,
which declines with age, is critical for immune function. An immunostatic mechanism exists that controls the proportions
of immune cell types, the production of cytokines and the level of expression of functional immune cell molecules.
309. Exposure to ionizing radiation is thought to affect T-cell homeostasis. Both experimental and epidemiological data have demonstrated that ionizing radiation may perturb T-cell homeostasis by reducing the ability of the immune system to produce new naive T-cells and by disturbing the regulation and maintenance of memory T-cell pools. A diverse pool of naive T-cells is necessary to produce immune responses to new antigens. Exposed atomic bombing survivors showed lower numbers of naive CD4+ and CD8+ T-cells. Although memory T-cell pools were either normal (CD4+) or even
larger (CD8+) in size [Y2], their TCR repertoire was significantly reduced with radiation dose [K25], probably due
to clonal expansion of memory T-cells. Alterations in T-cell subpopulations were also described in Chernobyl clean-up
workers [T6, Y4].
310. Radiation-induced perturbation of T-cell homeostasis may have important health implications. The reduction of the naive T-cell pool may lead to reduced ability of the host to defend against new pathogens, and the clonal expansion of memory T-cells associated with TCR repertoire deviation may compromise the ability of the host to control recurrent and latent infections [K36].
|
347. Besides apoptosis, which is a key mechanism within the immune system, it is rather difficult to classify the other mechanisms according to their importance after exposure to ionizing radiation. It likely that these mechanisms are interlinked, e.g. microscopic inflammation, propagated by a type of bystander mechanism and contributing to the ageing of tissues and promotion of cancer. Three hypotheses to further explore the mechanisms involved in the effects of ionizing radiation on the immune system and their impact in human health have been postulated by the Radiation Effects Research Foundation (RERF) (see section IV):
- Ionizing radiation may accelerate immunological ageing by perturbing T-cell homeostasis;
- Ionizing radiation may induce long-lasting inflammation that may lead to disease development;
- Individual immunogenetic background may determine individual susceptibility to succumbing to
disease.
348. Immune surveillance is different for the various cancer entities and has not been reported for all of them. The immune surveillance theory of cancer development remains controversial. Although the immune system has the capability to develop impressive antitumour effects, it is not very clear that cancer results from a deficiency of the immune system, and tumours can be promoted through low-level chronic inflammation because of alterations of immune cells. The potential effects of low doses of ionizing radiation on the critical balance existing in the immunological network (promoting or suppressing antitumour immunological response arising in the tumour microenvironment) has been insufficiently studied.
Erkrankungen durch ionisierende Strahlen außer Krebs:
Neuere Erkenntnisse über Effekte bei niedriger Dosis und chronischer Exposition
Teil 1: Herz-Kreislauf-Erkrankungen
Inge Schmitz-Feuerhake und Sebastian Pflugbeil
(Gesellschaft für Strahlenschutz e.V. und Bund zur Unterstützung Radargeschädigter e.V. Juli 2013)
"Seit den 1980er Jahren haben Kritiker auf die zahlreichen Einschränkungen hingewiesen, die
die Benutzung der japanischen Daten als Referenz für andere bestrahlte Kohorten mit sich
bringt, und die durchweg zu einer nennenswerten Unterschätzung der Folgen niedriger Dosen
bei Exposition einer normalen westeuropäischen Bevölkerung führt (Tabelle 1)."
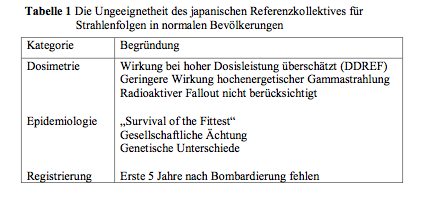
Quelle: Schmitz-Feuerhake und Pflugbeil (im Cache)
"Aufgrund der eindeutigen Befunde bei Beschäftigten der Nuklearindustrie
haben dann der unter Strahlenforschern bekannte Mathematiker Mark Little und sein Team
bestätigt, dass Strahlung bestimmte Blutkörperchen zerstört, die Entzündungen in den Arterien verhindern (Little 2009; Little 2010). Allgemein werden strahlenbedingte Gefäßveränderungen derzeit als Ursache kardiovaskulärer Erkrankungen angesehen (Hildebrandt 2010; Lee 2012). Eine andere These ist, dass strahlenbedingte Störungen der Nierenfunktion auf den
Kreislauf einwirken und zu dessen Versagen beitragen (Adams 2012)."
Adams, M.J., Grant, E.J., Kodama, K., Shimizu, Y., Kasagi, F., Suyama, A., Sakata, R., Akahoshi, M.:
Radiation dose associated wth renal failure mortality: a potential pathway to partially explain in-
creased cardiovascular disease mortality observed after whole-body irradiation. Radiat. Res. 177
(2012) 220-228
Hildebrandt, G.: Non-cancer diseases and non-targeted effects. Mutat. Res. 687 (2010) 73-77
Lee, M.O., Song, S.H., Jung, S., Hur, S., Asahara, T., Kim, H., Kwon, S.M., Cha, H.L.: Effect of ion-
izing radiation induced damage of endothelial progenitor cells in vascular regeneration. Arterioscler.
Thromb. Vasc. Biol. 32 (2012) 343-352
Little, M.P., Gola, A., Tzoulaki, I.: A model of cardiovascular disease giving a plausible mechanism
for the effect of fractionated low-dose ionizing radiation exposure. PloS. Comput. Biol. 2009
Oct;5(10):e1000539.Epub 2009 Oct 23
Little, M.P., Tawn, E.J., Tzoulaki, I., Wakeford, R., Hildebrandt, G., Paris, E., Tapio, S., Elliott, P.:
Review and meta-analysis of epidemiological associations between low/moderate doses of ionizing
radiation and circulatory disease risks, and their possible mechanisms. Radiat. Environ. Biophys. 49
(2010) 139-153
"Im Gegensatz zur ICRP, die zur Zeit auf einem "praktischen" Schwellenwert von 0,5 Sv beharrt, verfestigt sich in weiten Kreisen der Fachwelt die Erkenntnis, dass die Auswirkungen niedriger Dosen unterhalb dieses Wertes auf den Kreislauf ebenfalls relevant sind. Im November 2012 haben Little und 26 weitere Wissenschaftler aus verschiedenen Ländern eine Übersichtsarbeit dazu veröffentlicht."
Little, M.P., Azisova, T.V., Bazyka, D., Bouffier, S.D., Cardis, E., Chekin, S., Chumak, V.V., Cucinotta, F.A., de Vathaire, F., Hall, P., Harrison, J.D., Hildebrandt, G., Ivanow, V., Kasheev, V.V.,
Klymenko, S.V., Kreuzer, M., Laurent, O., Ozasa, K., Schneider, T., Tapio, S., Taylor, A.M., Tzoulaki, I., Vandoolaeghe, W.L., Wakeford, R., Zablotska, L.B., Zhang, W., Lipschultz, E.: Systematic
review and meta-analysis of circulatory disease from exposure to low-level ionizing radiation and
estimates of potential population mortality risks. Environ Health Perspect. 120 (2012) 1503-1511
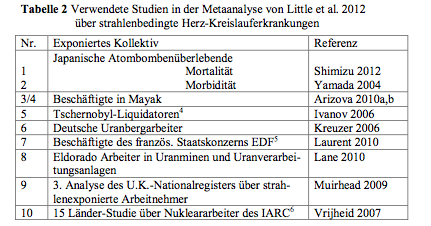
"Sie machten eine Literaturrecherche zum Thema ab 1990. Ihr vorläufiges Ergebnis ist, dass die strahlenbedingte Mortalität an Herz-Kreislauferkrankungen etwa so hoch ist wie diejenige durch strahlenbedingten Krebs. Die ausgewählten Studien sind in Tabelle 2 genannt."
4 Liquidatoren sind Personen, die am Unfallreaktor Abschirm- und Aufräumarbeiten versahen
5 Electricité de France
6 International Agency for Resarch on Cancer, eine Einrichtung der Weltgesundheitsorganisation WHO
Quelle: Schmitz-Feuerhake und Pflugbeil (im Cache)
Quelle: Schmitz-Feuerhake und Pflugbeil (im Cache)
|
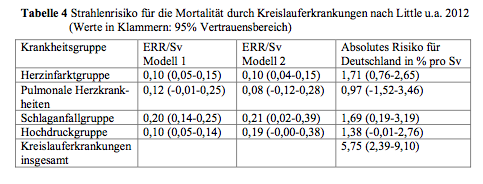
"Unter dem Relativen Risiko RR versteht man das Verhältnis der Erkrankungsrate in der exponierten Gruppe zur Erkrankungsrate in der Kontrollgruppe ohne Exposition. Hat das Relative Strahlenrisiko (RR pro Sv = RR/Sv) den Wert 2, ist die Erkrankungsrate in der exponierten Gruppe bei einer mittleren Dosis von 1 Sv genau doppelt so groß wie in der Kontrollgruppe.
... das "Excess Relative Risk" ERR = RR/Sv - 1.
Das Absolute Strahlenrisiko gibt die strahlenbedingte Erkrankungsrate pro Sv an, d.h. die
Anzahl der strahleninduzierten Fälle pro Anzahl Personen und Sv. ... Die Spontanrate oder anderweitig gewonnene Kontrollwerte
werden ... vorher abgezogen. Das Risiko für Krebstod bei Exposition einer Bevölkerung mit niedriger Dosis wird von der ICRP mit 5,5 % pro Sv [55 von 1000 Personen pro Sv] als absolutes Risiko angegeben (ICRP 2007).
ICRP, International Commission on Radiological Protection: The 2007 Recommendations of the International Commission on Radiological Protection. ICRP-Publication 103, Ann. ICRP 37 Nos. 2-4
(2007)
Es bedeutet, dass bei Bestrahlung einer Bevölkerung mit im Mittel 1 Sv dadurch 5,5 % der Personen einen strahlenbedingten Krebstod erleiden werden. Die von Little u.a. in der Metaanalyse erhaltenen Koeffizienten für das ERR wurden anhand
zweier statistischer Modellannahmen bestimmt."
|
Version: 17. Februar 2016
Adresse dieser Seite
Home
Joachim Gruber